NEJM Journal Watch Audio General Medicine
Guideline Watch: The Pendulum Swings Away from Aspirin for CVD Primary Prevention
June 01, 2022.Thomas L. Schwenk, MD, .Allan S. Brett, MD, .
Educational Objectives
Summary
Guideline Watch: The Pendulum Swings Away from Aspirin for Primary Prevention of Cardiovascular Disease
The U.S. Preventive Services Task Force (USPSTF) grading system has changed over time. In 1996, grade C was defined as “no recommendation for or against.” In 2002, grade A was defined as “strongly recommends the service.” From 2009 onward, definitions are as follows:
- Grade A: The USPSTF recommends the service. There is high certainty that the net benefit is substantial.
- Grade B: The USPSTF recommends the service. There is high certainty that the net benefit is moderate or there is moderate certainty that the net benefit is moderate to substantial.
- Grade C: The USPSTF recommends selectively offering or providing this service to individual patients based on professional judgment and patient preferences. There is at least moderate certainty that the net benefit is small.
- Grade D: The USPSTF recommends against the service. There is moderate or high certainty that the service has no net benefit or that the harms outweigh the benefits.
- Grade I: The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of the service.
The U.S. Preventive Services Task Force grade definitions are available (www.uspreventiveservicestaskforce.org/uspstf/about-uspstf/methods-and-processes/grade-definitions) free of charge.
Background
The potential value of aspirin for primary prevention of cardiovascular disease (CVD) first appeared in a 1989 recommendation by the USPSTF. During the years since 1989, subsequent iterations of the USPSTF guideline have varied in strength of recommendation, target age groups, and approach to balancing CVD benefit against bleeding risk.
History of U.S. Preventive Services Task Force Recommendations on Aspirin for Primary Prevention of Cardiovascular Disease
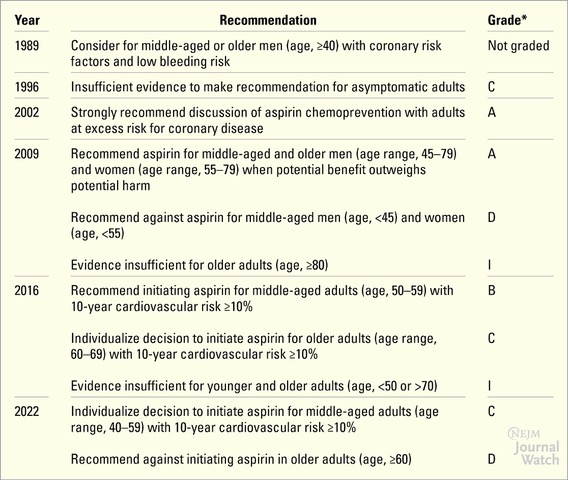
The Task Force broadened and strengthened its recommendation in 2009 and then weakened it in 2016. The pendulum now has swung further away from routine use of aspirin in the 2022 update that reflects results of three major randomized trials, published in 2018, that involved mostly older patients at moderate-to-high risk for CVD — ASPREE, ASCEND, and ARRIVE (https://www.jwatch.org/na47530 and N Engl J Med 2018; 379:1509; https://www.jwatch.org/na47393 and N Engl J Med 2018; 379:1529; and https://www.jwatch.org/na47429 and Lancet 2018; 392:1036). The latest recommendations (https://doi.org/10.1001/jama.2022.4983) and evidence report (https://doi.org/10.1001/jama.2022.3337) appear in the April 26, 2022 issue of JAMA.
Key Recommendations
- For middle-aged patients (age range, 40-59) with a 10-year risk for CVD ≥10%, the net benefit of aspirin use is small, but patients at low risk for bleeding might wish to consider initiating it (C recommendation).
- The USPSTF recommends against the initiation of aspirin use in older patients (age, ≥60; D recommendation).
In 13 years, the USPSTF has moved from a strong recommendation for aspirin use for primary prevention of CVD in a wide swath of adult patients to a weak recommendation for selective use only in patients at high risk for CVD and at low risk for bleeding (after a detailed shared decision-making discussion). One reason for this shift is the decline in absolute baseline risk for CVD due to the widespread application of other preventive strategies (i.e., antihypertensives, statins, and smoking cessation), leading to a smaller window of opportunity for benefit from aspirin, whereas risk for harm from bleeding has remained the same.
In an accompanying editorial (https://doi.org/10.1001/jama.2022.2460), Dr. Allan Brett discusses additional points. First, the recommendation statements only address initiating aspirin; the guideline does not directly address the issue of stopping aspirin therapy in patients when they reach the age of 60 or stopping it in longstanding aspirin users who now are presenting in their 60s or 70s. Although it makes intuitive sense to do so if one accepts the USPSTF position that net benefit disappears beyond age 60, stopping a preventive strategy once started is a different psychological decision than never starting it in the first place. The second issue is that the Task Force recommendation depends heavily on risk stratification derived from the American College of Cardiology/American Heart Association CVD risk calculator (https://www.cvriskcalculator.com/) that overpredicts risk in some populations. The seemingly objective, but actually imprecise, nature of the risk calculator presents significant challenges to both clinicians and patients in having productive shared decision-making discussions.
A close reading of the full USPSTF recommendation statement — and the evidence review that accompanies it — will provide helpful guidance for the patient-clinician discussions that inevitably will result from release of this recommendation.
Thomas L. Schwenk, MD & Allan S. Brett, MD
Dr. Brett wrote the editorial that accompanied this guideline in JAMA.
Readings
Disclosures
Acknowledgements
CME/CE INFO
Accreditation:
The Audio- Digest Foundation is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
The Audio- Digest Foundation designates this enduring material for a maximum of 0.00 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Audio Digest Foundation is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center's (ANCC's) Commission on Accreditation. Audio Digest Foundation designates this activity for 0.00 CE contact hours.
Lecture ID:
JW331113
Expiration:
This CME course qualifies for AMA PRA Category 1 Credits™ for 3 years from the date of publication.
Instructions:
To earn CME/CE credit for this course, you must complete all the following components in the order recommended: (1) Review introductory course content, including Educational Objectives and Faculty/Planner Disclosures; (2) Listen to the audio program and review accompanying learning materials; (3) Complete posttest (only after completing Step 2) and earn a passing score of at least 80%. Taking the course Pretest and completing the Evaluation Survey are strongly recommended (but not mandatory) components of completing this CME/CE course.
Estimated time to complete this CME/CE course:
Approximately 2x the length of the recorded lecture to account for time spent studying accompanying learning materials and completing tests.
More Details - Certification & Accreditation